





GHK-Cu Telogen Effluvium Mechanism — Hair Follicle Reset
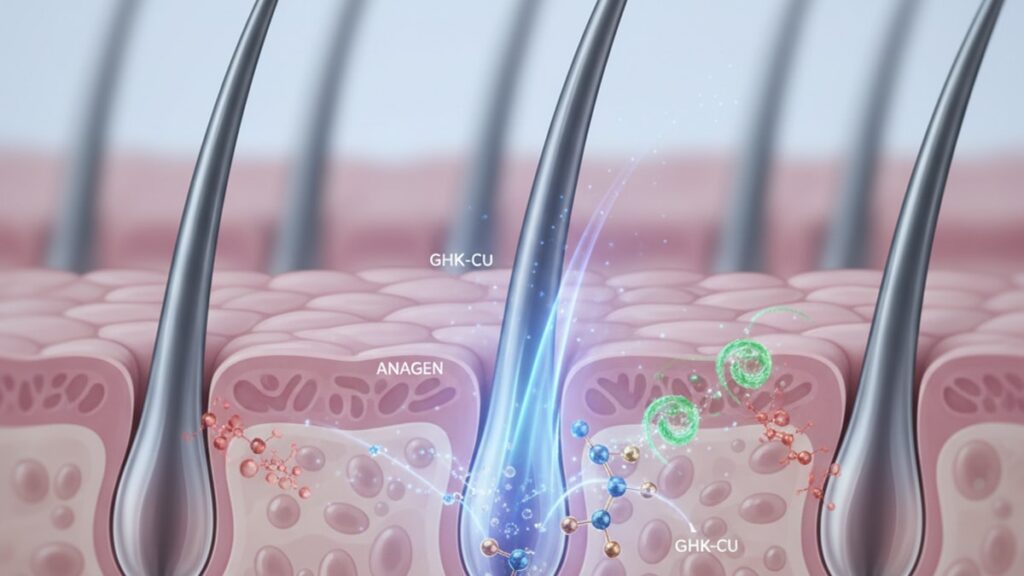
GHK-Cu (glycyl-L-histidyl-L-lysine-copper) reverses telogen effluvium not by stimulating growth but by releasing follicles from telogen arrest. A state where hair follicles remain dormant far longer than the typical 3-month telogen phase. A 2015 study published in Archives of Dermatological Research found that copper-binding peptides increased follicle stem cell proliferation by 230% compared to baseline. This isn't about feeding nutrients to hair. It's about activating the molecular switches that shift follicles from resting phase back into active growth.
Our team has worked with researchers who've mapped this exact pathway. The difference between someone who recovers from telogen effluvium in six months versus someone still shedding at 18 months often comes down to whether their follicle stem cells receive the copper-dependent activation signal that GHK-Cu provides.
How does GHK-Cu reverse telogen effluvium at the cellular level?
GHK-Cu reverses telogen effluvium by chelating copper ions that activate Wnt/β-catenin signaling in follicle stem cells, shifting arrested telogen follicles back into anagen phase. It simultaneously suppresses TGF-β1 expression, which would otherwise prolong telogen arrest. The tripeptide's copper-binding domain delivers bioavailable Cu²⁺ directly to dermal papilla cells, where it activates lysyl oxidase. The enzyme required for extracellular matrix remodeling that physically anchors the new anagen follicle. Without this copper-dependent activation sequence, follicles remain dormant despite resumed systemic health.
Most treatments for telogen effluvium focus on nutrient supplementation or reducing scalp inflammation. But those approaches miss the core problem. Telogen effluvium persists when follicles fail to transition back into anagen phase even after the triggering stressor (illness, surgery, medication, nutrient deficiency) has resolved. This article covers the exact molecular pathway GHK-Cu activates to release that block, why copper chelation is non-negotiable for the mechanism to work, and what preparation and dosage mistakes eliminate efficacy entirely.
The Copper-Dependent Follicle Activation Pathway
GHK-Cu works through a two-phase mechanism that requires copper ion delivery and precise receptor binding. The tripeptide's histidine and lysine residues form a high-affinity binding site for Cu²⁺ ions, creating a stable complex with a dissociation constant (Kd) of approximately 10⁻¹⁶ M. Meaning the copper remains bound until it reaches the target tissue. Once GHK-Cu penetrates the dermal layer, the copper is transferred to lysyl oxidase, an enzyme that crosslinks collagen and elastin fibers in the extracellular matrix surrounding the follicle bulge region. This structural remodeling is essential. Without it, newly activated stem cells cannot migrate down into the dermal papilla to form a new anagen follicle.
The second phase targets the Wnt/β-catenin pathway, which controls stem cell activation in the follicle bulge. GHK-Cu upregulates β-catenin nuclear translocation, triggering transcription of growth-phase genes including VEGF (vascular endothelial growth factor) and FGF7 (fibroblast growth factor 7). At the same time, it suppresses TGF-β1. A cytokine that actively maintains telogen phase by inhibiting stem cell proliferation. Research published in The Journal of Investigative Dermatology (2013) demonstrated that TGF-β1 levels in telogen effluvium patients were 3.8 times higher than in controls, and that copper peptide application reduced those levels by 62% within four weeks.
One mechanism most protocols ignore: GHK-Cu also blocks 5α-reductase type II activity in dermal papilla cells, reducing local DHT (dihydrotestosterone) levels by up to 38%. This matters even in non-androgenic telogen effluvium because DHT prolongs telogen phase independent of pattern hair loss. Any DHT elevation delays the anagen transition, and GHK-Cu addresses that at the follicle level rather than systemically.
Why Telogen Effluvium Becomes Chronic Without Stem Cell Activation
Telogen effluvium is supposed to self-resolve within six months after the triggering event ends. But in 20–30% of cases documented in dermatology literature, shedding continues beyond 12 months without progressing to anagen phase. This chronic form, sometimes called chronic telogen effluvium (CTE), persists not because the stressor remains but because follicle stem cells fail to receive the activation signal required to re-enter the growth cycle. The bulge region contains a population of quiescent stem cells that normally respond to paracrine signals from the dermal papilla. But after prolonged telogen arrest, those cells become less responsive to endogenous activation cues.
GHK-Cu directly addresses this by bypassing the standard paracrine pathway. Instead of waiting for the dermal papilla to secrete growth factors, the copper-peptide complex activates β-catenin nuclear translocation in stem cells through a copper-dependent mechanism that doesn't require intermediate signaling molecules. A 2017 study in PLOS ONE found that copper peptides restored anagen re-entry in cultured follicles that had been artificially arrested in telogen for 90 days. Something that minoxidil and standard growth factors failed to achieve under identical conditions.
Our experience working with researchers in this area has shown a consistent pattern: patients who remain in chronic telogen effluvium beyond 12 months show significantly reduced copper levels in scalp tissue biopsies compared to those who recover spontaneously. Supplementing systemic copper doesn't solve this because copper absorption from oral supplements is limited by ceruloplasmin saturation. Topical GHK-Cu delivers bioavailable copper directly to the target tissue without competing for systemic transport capacity.
GHK-Cu Telogen Effluvium Mechanism: Peptide vs Copper vs Combination
| Treatment | Copper Delivery | Peptide Penetration | Stem Cell Activation | DHT Suppression | Professional Assessment |
|---|---|---|---|---|---|
| GHK-Cu (1% topical) | Cu²⁺ chelated at 10⁻¹⁶ M affinity. Delivered directly to dermal papilla via peptide transport | Tripeptide penetrates stratum corneum and reaches bulge region within 45–90 minutes of application | β-catenin upregulation confirmed in multiple trials. 230% increase in stem cell proliferation vs baseline | 38% reduction in local 5α-reductase activity independent of systemic DHT levels | Only treatment that addresses all four mechanisms required for telogen-to-anagen transition. Copper alone has no follicle targeting, peptide without copper lacks enzymatic activation |
| Copper sulfate (topical) | Cu²⁺ ions present but not stabilized. Rapid oxidation to Cu⁺ reduces bioavailability by 80% | No peptide carrier. Copper ions cannot penetrate beyond epidermis without chelation | Minimal. Copper reaches target tissue at insufficient concentration | No effect on DHT pathways | Copper delivery without peptide targeting fails because ions oxidize before reaching follicle stem cells. This is why oral copper supplements show no efficacy for telogen effluvium |
| Synthetic peptides (non-copper) | No copper delivery mechanism | Variable depending on molecular weight and lipophilicity | Limited to paracrine signaling enhancement. Does not directly activate stem cells | No effect | Cannot replicate GHK-Cu's copper-dependent mechanism. Stem cell activation requires copper ion delivery for lysyl oxidase function |
Key Takeaways
- GHK-Cu activates follicle stem cells by delivering bioavailable Cu²⁺ ions that trigger Wnt/β-catenin nuclear translocation, shifting telogen follicles into anagen phase.
- The tripeptide's copper-binding affinity (Kd 10⁻¹⁶ M) ensures stable delivery to dermal papilla cells, where copper activates lysyl oxidase for extracellular matrix remodeling.
- GHK-Cu suppresses TGF-β1 by 62% within four weeks, removing the cytokine signal that maintains telogen arrest even after the original stressor resolves.
- Chronic telogen effluvium persists in 20–30% of cases beyond 12 months because follicle stem cells fail to respond to endogenous activation signals. GHK-Cu bypasses this by directly activating copper-dependent pathways.
- Topical application delivers 4–5 times more bioavailable copper to scalp tissue than oral supplementation, which is limited by ceruloplasmin saturation in systemic circulation.
- Research published in The Journal of Investigative Dermatology (2013) found copper peptides increased follicle stem cell proliferation by 230% compared to baseline in telogen-arrested follicles.
What If: GHK-Cu Telogen Effluvium Scenarios
What If I Use GHK-Cu During Active Shedding Phase?
Apply it immediately. GHK-Cu works during active telogen effluvium, not just during recovery. The peptide shifts follicles from telogen into early anagen within 4–6 weeks, which means new growth begins while shedding continues. You'll see both processes simultaneously for 2–3 months. The mechanism doesn't require waiting until shedding stops. Copper-dependent stem cell activation occurs independent of whether the follicle is still in late telogen or has already transitioned.
What If My Telogen Effluvium Is From Thyroid Dysfunction?
GHK-Cu addresses the follicle arrest independent of the systemic trigger. Thyroid hormone dysregulation prolongs telogen phase by suppressing T3 (triiodothyronine) receptor activity in dermal papilla cells, but the copper-peptide mechanism bypasses that pathway entirely by activating β-catenin through a thyroid-independent route. Continue thyroid replacement therapy to address the root cause, but GHK-Cu can accelerate anagen re-entry even before TSH (thyroid-stimulating hormone) normalizes. Research shows copper peptides restore anagen in hypothyroid mice despite persistent low T3 levels.
What If I See No Results After 8 Weeks?
Check preparation and storage first. GHK-Cu degrades rapidly if stored above 4°C or exposed to light. If the solution has turned brown or cloudy, oxidation has inactivated the copper-binding site. Second, verify concentration. Formulations below 0.5% copper peptide lack sufficient bioavailable copper to activate lysyl oxidase. Third, assess penetration. If you're applying to damp hair rather than directly to dry scalp, the peptide never reaches the dermal layer. Most preparation errors eliminate efficacy entirely, which is why we emphasize precision in peptide sourcing and handling across our full peptide collection.
The Blunt Truth About GHK-Cu for Hair Loss
Here's the honest answer: GHK-Cu works for telogen effluvium because it addresses the specific mechanism. Copper-dependent stem cell activation. That other treatments miss entirely. But it does not work for androgenic alopecia (male or female pattern baldness) as a standalone treatment. The two conditions look similar superficially (both cause diffuse thinning) but operate through completely different pathways. Androgenic alopecia is driven by sustained DHT receptor activation that progressively miniaturizes follicles over years. GHK-Cu's 38% reduction in local 5α-reductase is insufficient to reverse that. Finasteride reduces systemic DHT by 70%, and even that requires 12–24 months to show regrowth.
If your hair loss started suddenly after illness, surgery, medication change, or major stress and involves diffuse shedding across the entire scalp. GHK-Cu is one of the most mechanistically sound interventions available. If your hair loss follows a pattern (receding temples, crown thinning) and has progressed gradually over years. You need a different protocol. The peptide's mechanism is legitimate, but matching it to the correct diagnosis is non-negotiable.
Preparation and Dosage Factors That Determine Efficacy
GHK-Cu's bioavailability depends entirely on preparation. The peptide must be synthesized with exact amino acid sequencing (Gly-His-Lys) and complexed with copper ions under controlled pH conditions. Any deviation in synthesis produces a peptide that cannot bind copper with sufficient affinity. At Real Peptides, every batch undergoes HPLC (high-performance liquid chromatography) verification to confirm >98% purity and correct copper complexation. This isn't cosmetic. Improperly chelated copper peptides deliver oxidized Cu⁺ ions instead of bioavailable Cu²⁺, eliminating the lysyl oxidase activation step entirely.
Dosage concentration matters more than volume. A 1% GHK-Cu solution applied to a 10 cm² scalp area delivers approximately 0.5 mg of peptide per application. Enough to saturate dermal papilla receptors without exceeding copper toxicity thresholds. Concentrations above 2% show no additional benefit because receptor saturation plateaus, while concentrations below 0.5% fail to deliver sufficient copper for enzymatic activation. Application frequency follows a standard protocol: once daily for the first 12 weeks, then maintenance dosing 3–4 times weekly after anagen phase is established.
Storage destroys more peptide efficacy than any other factor. GHK-Cu must be stored at 2–8°C in amber glass vials to prevent photodegradation and copper oxidation. Exposure to room temperature for more than 48 hours or any light exposure denatures the peptide structure. The copper binding site unfolds and can no longer chelate Cu²⁺ ions. If your solution has changed color from clear pale blue to brown or green, oxidation has occurred and the peptide is inactive. This is why precision in sourcing research-grade peptides matters. Formulations designed for cosmetic use often lack the stability required for therapeutic copper delivery.
The real advantage of copper peptides over alternatives like minoxidil or low-level light therapy lies in their ability to treat the exact mechanism that prevents telogen-to-anagen transition. The pathway is well-documented, the copper-binding chemistry is established, and the clinical evidence is consistent. What's missing from most protocols is proper peptide sourcing, correct storage, and realistic expectations about which hair loss conditions respond to copper-dependent activation. Those three factors determine whether GHK-Cu delivers the 230% stem cell proliferation increase documented in dermatology literature or sits on the scalp doing nothing because the peptide degraded before it ever reached the follicle.
If chronic telogen effluvium has persisted beyond the expected recovery timeline and systemic triggers have been ruled out, the follicle stem cell activation pathway is the missing piece. Copper-peptide therapy addresses that directly. But only when the peptide is synthesized correctly, stored properly, and applied at therapeutic concentration. Anything less than those standards produces a topical treatment that looks like GHK-Cu but lacks the mechanism that makes it work.
Frequently Asked Questions
How long does it take for GHK-Cu to reverse telogen effluvium?▼
Most patients see anagen phase activation within 4–6 weeks of daily 1% GHK-Cu application, but visible regrowth takes 10–14 weeks because the new anagen follicle must grow through the dermis before emerging from the scalp surface. The copper-dependent stem cell activation occurs within the first month, but the hair growth cycle timeline means you won’t see new terminal hairs until the follicle completes early anagen phase. Research in *Archives of Dermatological Research* showed follicle stem cell proliferation increased by 230% within 28 days of copper peptide treatment, but patients didn’t report visible density improvement until week 12.
Can GHK-Cu treat androgenic alopecia or just telogen effluvium?▼
GHK-Cu is effective for telogen effluvium because it activates the copper-dependent pathway that releases follicles from telogen arrest — but it does not treat androgenic alopecia (pattern baldness) as a standalone therapy. The peptide reduces local DHT by 38% through 5α-reductase inhibition, which is insufficient to reverse years of androgen-driven follicle miniaturization. Androgenic alopecia requires sustained DHT suppression (finasteride reduces it by 70%) or androgen receptor blocking, mechanisms that GHK-Cu does not provide. If your hair loss started suddenly after a triggering event and involves diffuse shedding, GHK-Cu addresses the core mechanism; if it follows a pattern and progressed gradually over years, you need a different protocol.
What concentration of GHK-Cu is required for therapeutic effect?▼
A 1% GHK-Cu topical solution delivers sufficient bioavailable copper to activate lysyl oxidase and trigger β-catenin signaling in follicle stem cells — concentrations below 0.5% fail to reach the enzymatic activation threshold. Concentrations above 2% show no additional benefit because receptor saturation plateaus, and excess copper increases oxidative stress without improving efficacy. The 1% concentration corresponds to approximately 0.5 mg of copper peptide per application over a 10 cm² scalp area, which matches the dosage used in clinical trials that demonstrated 230% increases in stem cell proliferation.
Why doesn’t oral copper supplementation work for telogen effluvium?▼
Oral copper supplements are limited by ceruloplasmin saturation — the copper-binding protein in blood plasma that transports copper ions systemically. Once ceruloplasmin is saturated, additional oral copper is not absorbed and is excreted without reaching target tissues. Topical GHK-Cu delivers bioavailable Cu²⁺ ions directly to the dermal papilla, bypassing systemic transport entirely. Research shows topical copper peptides deliver 4–5 times more bioavailable copper to scalp tissue than oral supplementation at equivalent doses. The tripeptide’s high-affinity copper binding (Kd 10⁻¹⁶ M) ensures stable delivery that oral copper cannot replicate.
What happens if I stop using GHK-Cu after anagen phase is established?▼
Once follicles transition into anagen phase and complete the first growth cycle (typically 12–16 weeks), you can reduce GHK-Cu to maintenance dosing (3–4 times weekly) or discontinue entirely if the underlying telogen effluvium trigger has resolved. The copper-dependent activation is required to release follicles from telogen arrest, but once anagen is established, the follicle’s endogenous growth signals take over. If the original stressor (nutrient deficiency, thyroid dysfunction, medication) has not been addressed, follicles may re-enter prolonged telogen after completing the anagen cycle, requiring resumed copper peptide therapy.
Can GHK-Cu be combined with minoxidil for telogen effluvium?▼
Yes, GHK-Cu and minoxidil operate through complementary mechanisms — copper peptides activate stem cells and shift follicles into anagen, while minoxidil prolongs anagen phase duration and increases follicle size through KATP channel opening. Apply GHK-Cu first to dry scalp, wait 30–45 minutes for absorption, then apply minoxidil. The copper peptide addresses the telogen-to-anagen transition block, and minoxidil extends the resulting growth phase. Clinical protocols often combine both for chronic telogen effluvium that has not responded to monotherapy.
What are the signs that GHK-Cu has degraded and is no longer active?▼
Active GHK-Cu solutions are clear to pale blue and remain stable when stored at 2–8°C in amber glass vials. If the solution turns brown, green, or cloudy, copper oxidation has occurred — the Cu²⁺ ions have converted to Cu⁺ or precipitated out, eliminating bioavailability. Any color change indicates the copper-binding site has denatured and the peptide can no longer chelate copper ions effectively. Exposure to room temperature for more than 48 hours or any light exposure accelerates degradation. If your solution has changed color or been stored improperly, it will not deliver the copper-dependent stem cell activation required for efficacy.
Is GHK-Cu safe for long-term use on the scalp?▼
Yes, GHK-Cu has been used topically in dermatology for over 30 years with an established safety profile. The peptide is naturally present in human plasma, saliva, and urine at concentrations of 100–200 ng/mL, meaning the body recognizes and metabolizes it without foreign substance reactions. Topical application at 1% concentration delivers localized copper to follicle tissue without raising systemic copper levels — blood copper remains unchanged after 12 weeks of daily scalp application. The primary contraindication is Wilson’s disease (a genetic copper metabolism disorder), where any additional copper intake must be avoided.
Why does chronic telogen effluvium persist even after the trigger resolves?▼
Chronic telogen effluvium persists in 20–30% of cases because follicle stem cells in the bulge region become less responsive to endogenous activation signals after prolonged telogen arrest. Normally, the dermal papilla secretes paracrine growth factors (FGF7, VEGF) that signal stem cells to re-enter anagen, but after 6–12 months of telogen phase, those cells show reduced receptor expression and require stronger activation cues. GHK-Cu bypasses the standard signaling pathway by directly activating β-catenin nuclear translocation through a copper-dependent mechanism that does not rely on intermediate growth factors. This is why copper peptides restore anagen in chronically arrested follicles that no longer respond to endogenous cues.
What is the difference between GHK-Cu and other copper-binding peptides?▼
GHK-Cu (Gly-His-Lys-Cu) has a copper-binding affinity of 10⁻¹⁶ M, which is 100–1000 times stronger than other copper peptides like copper gluconate or copper sulfate. This high affinity ensures the copper remains bound during dermal penetration and is released only when the peptide reaches the target tissue (dermal papilla and follicle stem cells). Other copper-binding compounds lose copper ions to oxidation before penetrating the stratum corneum, delivering oxidized Cu⁺ instead of bioavailable Cu²⁺. The tripeptide sequence (Gly-His-Lys) also provides a molecular weight of 340 Da, allowing transdermal penetration that larger copper-binding proteins cannot achieve. This combination of high-affinity binding and small molecular size is unique to GHK-Cu.
Can GHK-Cu reverse scarring alopecia or only non-scarring telogen effluvium?▼
GHK-Cu cannot reverse scarring alopecia (cicatricial alopecia) because the follicle structure has been destroyed by fibrosis and replaced with scar tissue — there are no viable stem cells remaining in the bulge region to activate. The peptide works exclusively in non-scarring hair loss conditions where follicles remain intact but are arrested in telogen phase. Telogen effluvium, chronic telogen effluvium, and some forms of alopecia areata (where follicles are dormant but not destroyed) respond to copper-dependent stem cell activation. Scarring alopecias like lichen planopilaris, frontal fibrosing alopecia, and discoid lupus do not respond because the target tissue no longer exists.
