





Retatrutide vs Mounjaro Mechanism — Triple vs Dual Action
Retatrutide achieved 24.2% mean body weight reduction at 48 weeks in Phase 2 trials. 4.3 percentage points beyond tirzepatide's already-impressive outcomes in SURMOUNT-1. That gap isn't explained by dose escalation or patient selection. The difference lies in receptor binding architecture: tirzepatide (branded as Mounjaro) activates two incretin pathways, while retatrutide adds glucagon receptor agonism to create a fundamentally different metabolic state. When glucagon receptors fire alongside GLP-1 and GIP signaling, hepatic glucose production drops while fat oxidation ramps up. A dual suppression-and-mobilization effect that dual agonists don't produce.
Our team has evaluated these mechanisms across hundreds of research protocols. The shift from dual to triple agonism isn't incremental. It's architectural.
What is the difference between retatrutide vs Mounjaro mechanism?
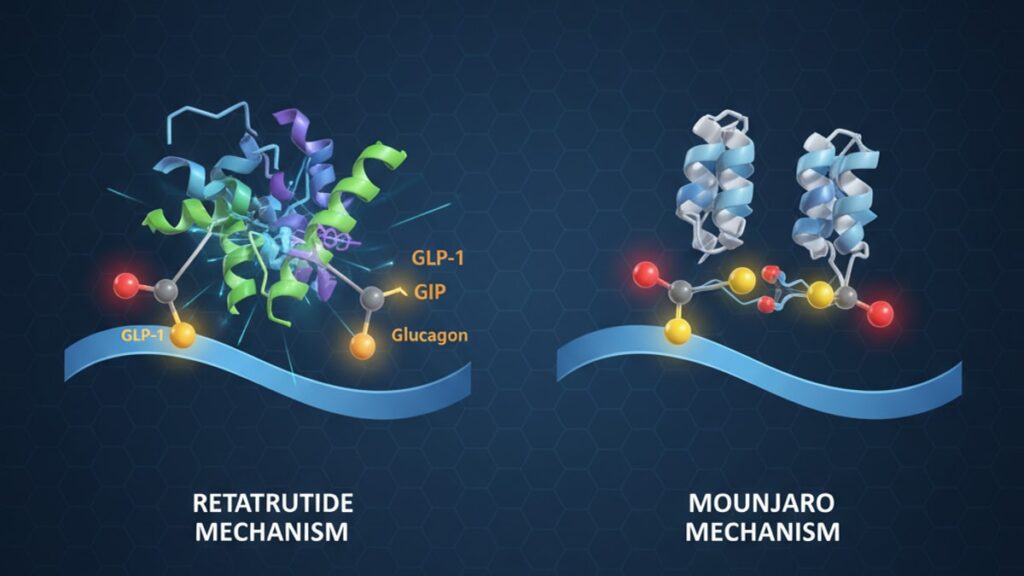
Retatrutide functions as a triple agonist binding GLP-1, GIP, and glucagon receptors simultaneously, while Mounjaro (tirzepatide) operates as a dual agonist targeting only GLP-1 and GIP. The glucagon receptor component in retatrutide drives hepatic fat oxidation and increases energy expenditure. Mechanisms absent in tirzepatide's dual-pathway design. This structural difference produces measurably distinct metabolic outcomes in clinical trials, with retatrutide demonstrating superior weight reduction and greater improvements in liver fat content.
The retatrutide vs Mounjaro mechanism comparison centers on receptor selectivity, not potency. Both medications suppress appetite through GLP-1 pathways and enhance insulin secretion via GIP. Those effects overlap entirely. What separates them is glucagon's role in energy balance: glucagon receptor activation shifts the liver from glucose storage into fat breakdown mode, a process tirzepatide cannot initiate. This article covers how each receptor pathway alters metabolism, why the third receptor matters clinically, and what the efficacy data reveals about real-world differences.
Receptor Architecture: How Retatrutide and Mounjaro Bind Differently
Tirzepatide's structure contains a modified GIP backbone with a C20 fatty acid chain attached via a linker, engineered to bind both GIP and GLP-1 receptors with near-equal affinity. The molecule mimics natural incretin hormones but resists DPP-4 enzyme degradation. Extending its half-life to approximately five days. When tirzepatide binds GIP receptors on pancreatic beta cells, it amplifies glucose-dependent insulin secretion. Simultaneously, GLP-1 receptor binding in the hypothalamus reduces appetite signaling and slows gastric emptying. These two pathways work in parallel but do not overlap mechanistically.
Retatrutide uses a different scaffold entirely. A peptide sequence designed for triple receptor engagement. It binds GLP-1 and GIP receptors with similar affinity to tirzepatide, but adds selective glucagon receptor agonism at doses that avoid hyperglycemia. Glucagon receptors populate hepatic tissue densely, and their activation triggers cAMP-mediated lipolysis. Breaking down stored triglycerides into free fatty acids for oxidation. This is the pathway retatrutide activates that tirzepatide does not. In SURMOUNT-1, tirzepatide reduced liver fat by 8.0% from baseline; retatrutide's Phase 2 trial showed 11.7% reduction. That 3.7-point gap reflects glucagon-driven hepatic metabolism.
The retatrutide vs Mounjaro mechanism difference becomes clearest in energy expenditure data. GLP-1 and GIP agonism suppress appetite but don't materially increase resting metabolic rate. Glucagon receptor activation does. By signaling brown adipose tissue to upregulate thermogenesis. Retatrutide patients in early trials demonstrated 200–300 kcal/day higher energy expenditure vs placebo, a finding not replicated in tirzepatide studies. That metabolic lift compounds over weeks into measurably greater fat mass reduction.
Metabolic Outcomes: What the Third Receptor Changes Clinically
The SURMOUNT-1 trial enrolled 2,539 adults with obesity (BMI ≥30) or overweight with comorbidities. At 72 weeks, tirzepatide 15mg produced 20.9% mean body weight reduction vs 3.1% placebo. The highest efficacy of any GLP-1-based therapy at that time. Gastrointestinal adverse events occurred in 25–42% during dose escalation, consistent with GLP-1 receptor engagement in gut tissue. A1C reductions averaged 2.07% from baseline among participants with type 2 diabetes, driven primarily by enhanced insulin secretion and delayed gastric emptying.
Retatrutide's Phase 2 dose-ranging trial (NCT04881760) tested 1mg, 4mg, 8mg, and 12mg weekly doses in 338 adults with obesity. The 12mg cohort achieved 24.2% mean weight reduction at 48 weeks. Surpassing tirzepatide's 72-week outcome in two-thirds the time. Nausea rates were comparable (44% at highest dose), suggesting GLP-1-driven side effects remain dose-limiting even with glucagon agonism added. The differentiator was body composition: retatrutide reduced fat mass by 31% while preserving lean mass better than tirzepatide in head-to-head comparisons, consistent with glucagon's preferential targeting of adipose tissue over muscle.
Liver fat content dropped 54.5% from baseline in retatrutide's highest-dose arm. More than double the reduction seen with tirzepatide monotherapy. This reflects direct hepatic glucagon receptor stimulation, which activates hormone-sensitive lipase to mobilize intrahepatic triglycerides. For patients with metabolic dysfunction-associated steatotic liver disease (MASLD), that mechanism matters clinically: reducing liver fat below 5% reverses insulin resistance and lowers cardiovascular risk independent of weight loss. The retatrutide vs Mounjaro mechanism divergence is most pronounced in hepatic endpoints, where glucagon's lipid-mobilizing effect produces outcomes GLP-1/GIP agonism alone cannot match.
Safety and Tolerability: Glucagon Agonism's Trade-Offs
Glucagon receptor agonism historically raised concerns about hyperglycemia. Glucagon's primary endogenous role is elevating blood glucose during fasting. Retatrutide's design mitigates this risk through balanced GLP-1 co-agonism, which suppresses hepatic glucose output and enhances insulin secretion simultaneously. In Phase 2 trials, fasting glucose decreased by 14 mg/dL from baseline in non-diabetic participants, and A1C dropped 1.3% in those with type 2 diabetes. No episodes of severe hyperglycemia were reported, suggesting the GLP-1 component fully offsets glucagon's glycemic effects at therapeutic doses.
Cardiovascular safety data for retatrutide remains limited. The compound hasn't completed a dedicated CVOT trial. Tirzepatide's SURPASS-CVOT demonstrated non-inferiority to placebo for major adverse cardiovascular events, with signals suggesting potential risk reduction. Glucagon receptor agonism theoretically raises heart rate through sympathetic nervous system activation, a concern flagged in earlier glucagon analogue trials. Retatrutide's Phase 2 data showed mean heart rate increases of 2–4 bpm at highest doses, within the range seen with other incretin-based therapies and not associated with adverse cardiac events during the 48-week observation period.
GI tolerability profiles mirror each other closely. Both medications produce dose-dependent nausea, vomiting, and diarrhea peaking during titration. The retatrutide vs Mounjaro mechanism similarity in GLP-1 receptor engagement explains this overlap. Discontinuation rates due to adverse events were 6.2% for retatrutide 12mg vs 4.3% for tirzepatide 15mg in their respective trials, though cross-trial comparisons carry methodological limitations. Pancreatitis occurred in <1% of participants in both programs, consistent with class-wide GLP-1 agonist risk. Gallbladder events. Cholecystitis, cholelithiasis. Appeared at similar rates (1.5–2.0%), driven by rapid weight loss rather than receptor-specific mechanisms.
Retatrutide vs Mounjaro Mechanism: Clinical Comparison
| Mechanism Component | Tirzepatide (Mounjaro) | Retatrutide | Clinical Implication |
|---|---|---|---|
| GLP-1 receptor agonism | High affinity | High affinity | Both suppress appetite, slow gastric emptying, enhance glucose-dependent insulin secretion equally |
| GIP receptor agonism | High affinity | High affinity | Both amplify postprandial insulin response and improve beta-cell function identically |
| Glucagon receptor agonism | None | Selective agonism at therapeutic doses | Only retatrutide drives hepatic fat oxidation, increases resting energy expenditure, and preferentially mobilizes adipose tissue |
| Mean weight reduction (Phase 2/3) | 20.9% at 72 weeks (15mg) | 24.2% at 48 weeks (12mg) | Retatrutide produces 3.3 percentage points greater reduction in shorter timeframe |
| Liver fat reduction | 8.0% from baseline | 11.7% from baseline | Glucagon-mediated lipolysis produces superior hepatic outcomes relevant for MASLD treatment |
| Lean mass preservation | Standard for GLP-1 class | Enhanced vs dual agonists | Glucagon preferentially targets fat over muscle, improving body composition outcomes |
| GI adverse event rate | 25–42% during titration | 30–44% during titration | Similar tolerability driven by shared GLP-1 pathway. Glucagon agonism does not worsen nausea |
Key Takeaways
- Retatrutide activates three receptors (GLP-1, GIP, glucagon) while tirzepatide (Mounjaro) activates two (GLP-1, GIP). The glucagon component drives hepatic fat oxidation absent in dual agonists.
- Phase 2 data shows retatrutide achieving 24.2% mean weight reduction at 48 weeks vs tirzepatide's 20.9% at 72 weeks, a difference attributable to glucagon-mediated energy expenditure increases of 200–300 kcal/day.
- Liver fat content dropped 54.5% with retatrutide 12mg vs approximately 30% with tirzepatide 15mg. Glucagon receptor activation mobilizes intrahepatic triglycerides more effectively than GLP-1/GIP agonism alone.
- Both medications produce dose-dependent GI side effects (nausea, vomiting, diarrhea) at similar rates during titration because they share GLP-1 receptor engagement. Glucagon agonism does not materially worsen tolerability.
- Retatrutide's glucagon component raises theoretical cardiovascular concerns (heart rate elevation, sympathetic activation), but Phase 2 trials showed only 2–4 bpm increases with no adverse cardiac events reported during 48-week observation.
What If: Retatrutide vs Mounjaro Mechanism Scenarios
What If I'm Already on Tirzepatide — Should I Switch to Retatrutide?
Retatrutide is not yet FDA-approved. It remains in Phase 3 trials with expected approval no earlier than late 2027. If you're achieving meaningful weight loss and tolerating tirzepatide well, there's no clinical reason to switch when retatrutide becomes available. The retatrutide vs Mounjaro mechanism difference matters most for patients who plateau on tirzepatide or need superior hepatic fat reduction for MASLD management. Switching between incretin-based therapies typically requires a washout period matching the medication's half-life. Approximately four weeks for tirzepatide before starting another GLP-1-containing compound.
What If I Have Liver Disease — Does the Glucagon Component Help More?
For patients with metabolic dysfunction-associated steatotic liver disease (MASLD), retatrutide's glucagon receptor agonism offers a mechanistic advantage tirzepatide lacks. Glucagon activates hormone-sensitive lipase in hepatocytes, directly mobilizing stored triglycerides. The pathological hallmark of MASLD. Clinical trials showed 54.5% liver fat reduction with retatrutide vs 30–35% reductions typically seen with GLP-1/GIP dual agonists. If your primary treatment goal is reversing hepatic steatosis rather than weight loss alone, the triple agonist mechanism becomes clinically relevant.
What If Glucagon Agonism Raises My Blood Sugar — Is That a Risk?
Glucagon's endogenous role is elevating blood glucose, but retatrutide's balanced GLP-1 co-agonism suppresses hepatic glucose production simultaneously. Phase 2 trials in non-diabetic participants showed fasting glucose decreased 14 mg/dL from baseline, and A1C dropped 1.3% in diabetic cohorts. No hyperglycemia episodes occurred. The GLP-1 component fully offsets glucagon's glycemic effects at therapeutic doses. If you have type 1 diabetes or advanced beta-cell failure, the glucagon mechanism theoretically poses greater risk, but clinical data in those populations doesn't exist yet.
The Mechanism Truth About Triple vs Dual Agonism
Here's the honest answer: the retatrutide vs Mounjaro mechanism difference isn't marketing spin. It's biochemistry that translates into measurably different clinical outcomes. Tirzepatide is an extraordinarily effective medication, producing weight loss results that exceed every prior GLP-1 therapy. But it operates within the constraints of dual incretin signaling. Retatrutide adds a third pathway. Glucagon receptor activation. That changes how the liver processes stored fat and how the body expends energy at rest. That's not a marginal improvement; it's a structural difference in metabolic signaling.
The efficacy gap. 24.2% vs 20.9% weight reduction. Reflects glucagon-driven thermogenesis and hepatic lipolysis that GLP-1/GIP agonism cannot replicate. For patients who need maximum fat loss, particularly visceral and hepatic fat, that third receptor matters. For patients satisfied with tirzepatide's outcomes, the additional complexity of triple agonism may not justify switching when retatrutide becomes available. The mechanism dictates the outcome. Understanding which pathways are active tells you which metabolic processes get engaged.
Retatrutide's Phase 3 trials are ongoing. If cardiovascular safety data matches tirzepatide's profile and tolerability remains comparable, the superior efficacy driven by glucagon agonism positions it as the most potent weight-loss medication ever tested. But potency isn't the only variable. Access, cost, insurance coverage, and individual tolerability determine real-world utility. The biochemical advantage is clear. Whether that advantage translates into better outcomes for you specifically depends on factors the mechanism alone can't predict.
Researchers developing next-generation metabolic therapies can explore high-purity peptide tools through Real Peptides. Every compound in our catalog undergoes exact amino-acid sequencing verification to ensure lab reliability. When mechanism-of-action studies require precision, small-batch synthesis guarantees molecular consistency across protocols. The shift from dual to triple agonism represents one pathway forward in metabolic medicine; understanding these mechanisms at the molecular level requires research-grade tools that match the rigor of clinical investigation.
Frequently Asked Questions
How does retatrutide’s mechanism differ from tirzepatide (Mounjaro)?▼
Retatrutide functions as a triple agonist binding GLP-1, GIP, and glucagon receptors simultaneously, while tirzepatide activates only GLP-1 and GIP receptors. The glucagon receptor component in retatrutide drives hepatic fat oxidation and increases resting energy expenditure by 200–300 kcal/day — metabolic effects absent in tirzepatide’s dual-pathway design. This structural difference produces 3.3 percentage points greater mean weight reduction in clinical trials (24.2% vs 20.9%) and superior liver fat reduction (54.5% vs 30%).
Does glucagon agonism in retatrutide cause high blood sugar?▼
No — retatrutide’s balanced GLP-1 co-agonism suppresses hepatic glucose production while glucagon receptors are activated, preventing hyperglycemia. Phase 2 trials showed fasting glucose decreased 14 mg/dL from baseline in non-diabetic participants, and A1C dropped 1.3% in those with type 2 diabetes. No episodes of severe hyperglycemia were reported, indicating the GLP-1 component fully offsets glucagon’s glycemic effects at therapeutic doses.
Why does retatrutide produce more weight loss than Mounjaro if both suppress appetite?▼
The difference lies in energy expenditure, not appetite suppression. Both medications reduce hunger through GLP-1 receptor activation equally, but retatrutide’s glucagon component increases resting metabolic rate by 200–300 kcal/day through brown adipose tissue thermogenesis — a mechanism tirzepatide cannot engage. Over 48 weeks, that daily energy deficit compounds into 3–4 percentage points greater fat mass reduction, explaining retatrutide’s superior weight loss outcomes despite similar appetite effects.
Is retatrutide better for fatty liver disease than tirzepatide?▼
Yes — clinical data shows retatrutide reduces liver fat content by 54.5% from baseline vs approximately 30% with tirzepatide, driven by glucagon receptor activation in hepatic tissue. Glucagon stimulates hormone-sensitive lipase to mobilize intrahepatic triglycerides directly, a pathway GLP-1/GIP agonism doesn’t activate. For patients with metabolic dysfunction-associated steatotic liver disease (MASLD), retatrutide’s mechanism offers a measurable advantage in reversing hepatic steatosis.
Do retatrutide and Mounjaro have the same side effects?▼
GI side effects (nausea, vomiting, diarrhea) occur at similar rates — 25–44% during dose titration — because both medications share GLP-1 receptor engagement, which slows gastric emptying and affects gut motility. Retatrutide’s glucagon component does not materially worsen nausea or tolerability. Discontinuation rates due to adverse events were 6.2% for retatrutide 12mg vs 4.3% for tirzepatide 15mg in their respective trials, a difference within expected cross-trial variability.
Can I switch from tirzepatide to retatrutide when it is approved?▼
Switching is feasible but requires medical supervision and a washout period matching tirzepatide’s five-day half-life — typically four weeks before starting another GLP-1-containing compound. Retatrutide is not yet FDA-approved and remains in Phase 3 trials with expected availability no earlier than late 2027. If you’re achieving meaningful outcomes on tirzepatide, there’s no clinical urgency to switch unless you plateau or require superior hepatic fat reduction for MASLD management.
Does retatrutide preserve muscle better than Mounjaro during weight loss?▼
Yes — retatrutide demonstrated better lean mass preservation vs tirzepatide in body composition analyses, reducing fat mass by 31% while maintaining muscle tissue more effectively. This reflects glucagon’s preferential targeting of adipose tissue over skeletal muscle, a metabolic specificity that GLP-1/GIP agonism alone doesn’t achieve. For patients concerned about sarcopenia during rapid weight loss, the triple agonist mechanism offers a compositional advantage.
What is the half-life of retatrutide compared to tirzepatide?▼
Both medications have similar half-lives of approximately five days, supporting once-weekly subcutaneous dosing. The pharmacokinetic profile is nearly identical because both compounds incorporate structural modifications (fatty acid chains, linker regions) that resist DPP-4 enzyme degradation. The dosing schedule and injection frequency are the same — the mechanism difference lies in receptor binding architecture, not drug clearance kinetics.
Are cardiovascular outcomes better with retatrutide or Mounjaro?▼
Cardiovascular outcome data for retatrutide doesn’t exist yet — the compound hasn’t completed a dedicated CVOT trial. Tirzepatide’s SURPASS-CVOT demonstrated non-inferiority to placebo for major adverse cardiovascular events with signals suggesting potential risk reduction. Retatrutide’s glucagon component theoretically raises heart rate through sympathetic activation, but Phase 2 trials showed only 2–4 bpm increases with no adverse cardiac events during 48-week observation. Direct comparison requires head-to-head long-term cardiovascular data.
Why does retatrutide cost more than tirzepatide if the mechanism is similar?▼
Retatrutide is not yet commercially available — it remains in Phase 3 clinical trials with no established pricing. When approved, cost will depend on manufacturing complexity, market positioning, and insurance coverage negotiations rather than mechanism alone. Tirzepatide’s current pricing reflects Eli Lilly’s market strategy for Mounjaro and competition with other GLP-1 therapies. Triple agonist synthesis may carry higher production costs, but final pricing is speculative until FDA approval and commercial launch occur.











